 |
| Service Delivery Model of Health Promotion for People with Disabilities |
Figure 1 Click here to view larger image
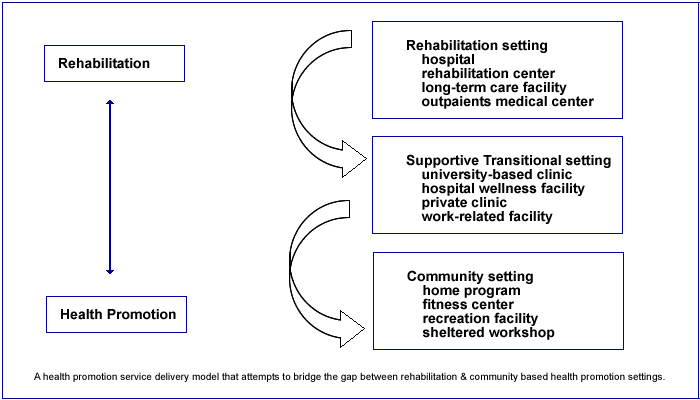
Figure 1 illustrates a health promotion service delivery model that attempts to bridge the gap between Rehabilitation and Community-Based Health Promotion. Because most rehabilitation programs are often short-term in nature and have a primary emphasis on acute care (i.e., treating an injury or illness), there is usually not enough time available to complete treatment and simultaneously provide a comprehensive health promotion program. The Supportive Transitional Setting is used to transition the person from rehabilitation to community-based health promotion and offers the individual a more holistic approach to managing their health using the core domains of exercise, nutrition and health education. The person can also continue their rehabilitation in this setting, if necessary, and focus on the areas of health promotion that will help reduce the occurrence of a similar injury or secondary condition.
The Supportive Transitional Setting is also available to persons with disabilities who have not been in rehabilitation but would like to begin a health promotion program. Since most health professionals lack the resources and knowledge on how to adapt or modify health promotion programs for people with disabilities, the Supportive Transitional Setting provides a place where individuals can learn how to manage their own health. Participants are taught how to overcome environmental barriers to participation and learn how to maintain their own health independently or with minimal assistance. For example, individuals who have had a stroke will often need to learn how to monitor their own blood pressure, know the warning signs for when to stop exercising, and understand what type of foods may be restricted if they are taking the blood thinner, Coumadin. Persons with stroke may also need to be taught how to mount and dismount a stationary cycle to avoid falling, or may need some type of low-tech adaptation to prevent their foot from slipping off the pedal. This information is extremely important to provide the participant before they enter the Community Setting where there may be minimal or no supervision and a lack of knowledge on how to adapt or modify programs to meet their specific needs.
The major emphasis of the Supportive Transitional Setting is to empower people with disabilities to take greater control of their own health and to know what types of services to request when they enroll in a community-based program. The participant is also provided with a number of home-based remedies for improving health, including adapted exercises that do not require expensive equipment, healthy recipes that fit within the person's budget and are culturally sensitive, a listing of foods that may interact with certain medications, and relaxation techniques for coping with stressful events or pain. The other unique feature of the Supportive Transitional Setting is that it uses a group format to teach individuals with disabilities good health maintenance practices. The group format allows individuals to interact with each other and often results in new friendships that serve as a social support mechanism during and after the program.
The bidirectional arrows illustrated in the model imply that at various times in the person's life it may be necessary to return to the rehabilitation setting for a new or recurring injury or secondary condition (e.g., fall-related injury, loss of function, pressure sore). After rehabilitation, the person may choose to return to the Supportive Transitional Setting to learn new techniques or strategies for avoiding a similar injury or secondary condition, or they can reenter at the Community level and manage their own health. Programs in the Supportive Transitional Setting can vary in length from several weeks to several months depending on the needs of the individual and their readiness to engage in health promoting behaviors on their own volition.